
Women's Libido Telemedicine: Why Desire Drops and What Actually Helps
Low sexual desire in women, known clinically as hypoactive sexual desire disorder or HSDD, is the most common female sexual health complaint in the United States. Research using the PRESIDE study found it affects roughly 8.9% of women ages 18 to 44 and 12.3% of women ages 45 to 65, and it is treatable once the actual cause is identified. Women's libido telemedicine has become one of the more searched paths to that evaluation, mostly because the alternative, a rushed conversation at a yearly exam or a months-long wait for a specialist, has never worked well for a topic this personal.
You already know the version of this that does not get talked about. It is 11pm, the kids are finally asleep, and you are quietly searching on your phone instead of asking your doctor at your last appointment, again. You are not confused about what is happening. You noticed months ago. What you have not done yet is find out why, mostly because the "why" always seemed obvious enough to not bother asking.
That assumption is worth examining, because it is usually the thing standing between a woman and an actual answer.
What Counts as a Real Drop in Desire

Clinically, HSDD is defined as a persistent or recurrent lack of sexual thoughts, fantasies, or desire that causes personal distress, lasting six months or longer, according to the International Society for the Study of Women's Sexual Health (ISSWSH) expert consensus panel. That word, distress, is the entire diagnostic hinge. A naturally lower baseline desire that does not bother you is not a disorder. A level of desire that used to feel normal to you, that has now dropped, and that you find genuinely upsetting, is something a clinician would take seriously.
Providers also separate HSDD into a few categories that matter for treatment:
Generalized vs. situational. Generalized means low desire in every context. Situational means desire is fine in some circumstances but not others, often pointing toward a relationship or environmental cause rather than a biological one.
Lifelong vs. acquired. Lifelong means desire has always been lower than a woman would like. Acquired means something changed, which usually points investigators toward a specific trigger: a new medication, a hormonal shift, a life event.
Did you know? The FDA's own review of clinical trial data for flibanserin estimated that HSDD affects 7.7% to 14% of premenopausal American women, or an estimated 5.5 to 8.6 million women ages 20 to 49. It is common enough that most primary care providers will have already had this exact conversation dozens of times.
The Attribution Trap: Why Most Women Wait Years to Ask About This

There is a specific reasoning pattern that keeps women from bringing this up, and it has nothing to do with embarrassment. Psychologists call it an attribution error: the tendency to assign a single, obvious explanation to a problem and then stop investigating, even after that explanation should have run its course.
It usually goes like this. Desire drops. A woman correctly identifies a plausible cause: new baby, new antidepressant, a stretch of work stress, the exhaustion of caregiving. She files the problem under that cause and waits for it to resolve on its own. Eighteen months later, the baby is sleeping through the night, the stressful project ended, and the desire has not come back. But because the original explanation felt so reasonable, she never revisits the question of whether something else, something biological, was contributing the whole time.
This matters clinically because several of the most common causes of acquired HSDD (perimenopausal hormone shifts, SSRI-induced sexual side effects, undiagnosed thyroid dysfunction) look, from the inside, exactly like ordinary life stress. They do not announce themselves. The only way to tell the difference is to actually ask a provider, which is the step the attribution trap quietly talks women out of.
Expert insight: Based on the volume of women's health visits our platform sees, the most common line providers hear is some version of "I thought it would go back to normal once things calmed down." It rarely does on its own when there is a hormonal or medication-related cause underneath. That is not a failure of willpower. It is a workup that never happened.
What Is Actually Behind Low Libido

There is rarely one single cause. Most women who get a proper evaluation find two or three overlapping factors.
Hormonal changes
Estrogen and testosterone both decline through perimenopause and menopause, and both play a role in desire, arousal, and vaginal comfort. Postpartum hormone shifts and thyroid dysfunction (both hypothyroidism and hyperthyroidism) are also well-documented contributors, according to the American Sexual Health Association.
Medication side effects
This is the most underdiagnosed category. SSRIs and SNRIs, including sertraline, paroxetine, escitalopram, fluoxetine, and venlafaxine, are well known to reduce desire and delay orgasm, with paroxetine carrying the highest documented risk of the group, per Mayo Clinic. Some hormonal birth control formulations and certain blood pressure medications can have a similar effect.
The depression connection itself
Depression lowers libido independently of any medication, through the same neurochemical pathways that flatten mood and motivation more broadly. We have written before about how depression and anxiety influence physical health in ways people do not expect, and sexual desire is one of the clearest examples.
Relationship and situational factors
Conflict, mismatched schedules, and unresolved resentment are real contributors, particularly in situational HSDD where desire is intact in other contexts.
Underlying medical conditions
Diabetes, pelvic pain conditions like endometriosis, and genitourinary syndrome of menopause (vaginal dryness and thinning that makes sex physically uncomfortable) can all suppress desire indirectly, simply because the brain learns to avoid something that hurts or feels difficult.
Common mistake to avoid
Assuming a single cause and stopping there, especially "it's just stress" or "it's just my antidepressant." Both may be true and still not be the whole picture. A provider who reviews your full medication list, symptom timeline, and menstrual or menopausal status will usually find more going on than the first, most obvious explanation.
What Waiting Actually Costs You

Hormonal decline in perimenopause is progressive, not static, and some causes are genuinely easier to address earlier. Medication-induced sexual dysfunction from an SSRI, for example, is a straightforward adjustment with your provider (a dose change, a different medication, or an added medication) but only if you say something. Left unaddressed, one of the most common outcomes is that women quietly stop taking an antidepressant that is otherwise working, on their own, without medical guidance, simply to get their sex life back. That trade is rarely necessary once a provider knows what is happening.
The relational cost is also real and rarely discussed directly. Unaddressed low desire is consistently associated with lower reported relationship satisfaction and general happiness, according to ISSWSH's review of the research, independent of whether a couple ever explicitly discusses it.
How Telemedicine Evaluates and Treats Low Libido

A telehealth visit for low libido follows roughly the same clinical logic as an in-person one, minus the waiting room.
Symptom and history intake. You describe when the change started, whether it is generalized or situational, and what else was happening in your life at the time.
Medication review. Your provider checks your current prescriptions, particularly antidepressants, blood pressure medications, and hormonal birth control, for known sexual side effects.
Screening for underlying causes. This includes menopausal status, thyroid symptoms, mood symptoms, and relationship context. Lab work, such as a thyroid panel or hormone panel, may be ordered if indicated.
A treatment plan appropriate to the cause, which may include:
An FDA-approved medication for HSDD, if you meet the clinical criteria
A medication adjustment if an antidepressant is the likely cause
Off-label testosterone therapy, for postmenopausal women, dosed and monitored according to the Global Consensus Position Statement on testosterone therapy for women, endorsed by ten international menopause, endocrine, and sexual medicine societies
A referral for vaginal estrogen therapy if genitourinary symptoms are the primary driver
A referral to a sex therapist or counselor if the cause is primarily relational
An in-office equivalent of this same evaluation, especially one that includes a referral to a gynecologist or endocrinologist, commonly costs several hundred dollars before any treatment is even started. A $20 virtual women's health visit covers the same initial evaluation and, when clinically appropriate, the prescription itself.
Addyi vs Vyleesi: Comparing the Two FDA-Approved Options
Two medications currently carry an FDA indication specifically for HSDD. As of December 2025, the FDA approved an expanded indication for flibanserin (Addyi) to include postmenopausal women under 65, in addition to its original premenopausal indication. This is a recent and meaningful change: for a decade, postmenopausal women had no FDA-approved medication option at all for this specific condition.
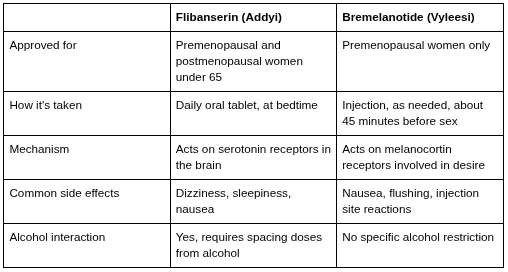
Both medications require a clinical evaluation to confirm the diagnosis fits (acquired, generalized HSDD not better explained by a relationship problem, another medication, or an untreated medical or psychiatric condition), which is exactly what a telehealth intake is designed to screen for, per GoodRx's clinical comparison of the two drugs.
Pro tip: If an antidepressant is a likely contributor to your symptoms, mention it clearly in your intake. Neither Addyi nor Vyleesi is intended to treat medication-induced sexual side effects, and your provider will likely start by addressing the medication itself, often by adjusting the dose or switching to an option with a lower sexual side effect profile, such as bupropion, rather than adding a second prescription on top.
Is a $20 Telehealth Visit a Legitimate Way to Get This Evaluated

This is the honest question underneath most searches like this one, and it deserves a direct answer: yes, for the initial evaluation, medication review, and prescribing of non-controlled medications like flibanserin, telehealth is an appropriate and increasingly standard first step. It is not a shortcut around real care. It is the same clinical questions asked by the same category of licensed provider, delivered without an appointment, a referral, or a waiting room.
Practical Telehealth was founded by Casey Hicks, a board-certified Family Nurse Practitioner, specifically because these kinds of conversations, the ones patients defer for months because the traditional system makes them harder than they need to be, deserve a faster and more private front door. Every visit is reviewed by a licensed provider, and the platform does not prescribe controlled substances. Flibanserin and bremelanotide are both non-controlled, which is part of why this particular condition is well suited to virtual evaluation.
When You Need an In-Person Provider Instead

Telehealth is genuinely the wrong tool in a few specific situations, and a good provider will say so rather than force a virtual fit:
New pelvic pain, unusual bleeding, or a suspected structural issue that needs a physical exam
Symptoms that suggest a condition requiring imaging or in-office testing
Vyleesi specifically, since it is a subcutaneous injection that some women prefer to learn to self-administer with hands-on guidance first
A telehealth visit is still useful in these cases as a first step. It can identify that an in-person referral is needed faster than waiting for the next available specialist appointment would.
FAQs
What is considered low libido in women?
Low libido becomes a clinical concern, specifically HSDD, when a persistent lack of sexual desire lasts six months or longer and causes you personal distress. A naturally lower desire that does not bother you is not considered a disorder.
Is low sex drive in women a real medical condition?
Yes. HSDD is recognized by the International Society for the Study of Women's Sexual Health and is estimated to affect close to 1 in 10 adult women in the United States, making it the most common female sexual health complaint.
Can telemedicine prescribe Addyi or Vyleesi?
A licensed telehealth provider can evaluate whether you meet the clinical criteria for either medication and prescribe flibanserin (Addyi) if appropriate, since it is a non-controlled oral medication. Bremelanotide (Vyleesi) is a self-injected medication, so your provider may recommend an in-person visit for initial administration guidance.
Does testosterone help women's libido?
For postmenopausal women, testosterone therapy at physiologic, monitored doses has shown benefit for HSDD and is endorsed by the Global Consensus Position Statement, backed by ten international medical societies. It is used off-label in the United States, since no testosterone product is currently FDA-approved specifically for women.
Can antidepressants cause low libido, and can telehealth help with that?
Yes. SSRIs and SNRIs are among the most common causes of medication-induced low libido. A telehealth provider can review your current antidepressant, discuss dose adjustments or alternative medications with a lower sexual side effect profile, and coordinate care without you needing to stop your medication on your own.
How much does a telehealth visit for low libido cost at Practical Telehealth?
A visit is a flat $20, with no insurance required. That covers the intake review and provider evaluation; any prescribed medication is billed separately through your pharmacy.
Is menopause the main cause of low libido?
It's a major contributor for many women, since estrogen and testosterone both decline during this transition, but it is rarely the only factor. Medication side effects, thyroid function, mood, and relationship context all need to be considered for an accurate picture.